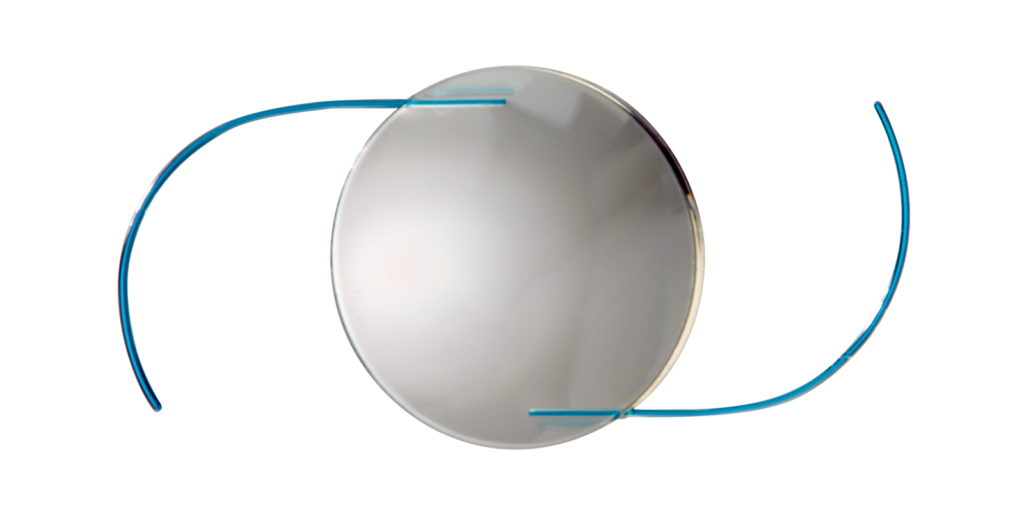
PanOptix Trifocal dominates Cataract Philadelphia
Enjoy a glasses-free life, with the most advanced multifocal IOL.
Alcon's PanOptix implant, a second generation trifocal, provides continuous focus without glasses for tasks like driving, reading and computer use. PanOptix has been available outside the US for a dozen years and it is driving the premium intraocular lens markets in Canada, Australia and Europe. Our practice uses advanced intraocular lens power calculation methods to select the ideal PanOptix implant for appropriate patients.
RxSight Light Adjustable Lens
Select uncompromised clarity with an IOL that matches your visual requirements.
RxSight's Light Adjustable Lens (LAL) is customized to your needs. Former LASIK patients achieve the WOW they remember. Monovision patients achieve sharp driving and personalized near vision. Perfectionist obtain the clearest vision without glasses. Adjustments are done at our Elkins Park office. We were the first and remain the most experienced practice in Pennsylvania to offer this incredible technology. Test drive the LAL and define your visual success.

AcrySof IQ Vivity
Designed to deliver an extended focal range and a monofocal-like visual disturbance profile.
Vivity uses non-diffractive optics to achieve an excellent range of vision without loss of contrast sensitivity or glare at night. Patients who are not ideal candidates for a trifocal implant can enjoy superior visual function with this lens. Vivity’s innovative technology brings premium visual results to more patients.

Dropless and Less Drops Cataract Surgery
Choose safer surgery, save $100 to $300 per eye, and reduce the hassle of multiple eye drops.
Intraocular antibiotics administered at the time of eye surgery reduces risk. We have employed this technique successfully on 14,000 cases since 2014. By instilling antibiotics and steroids in the operating suite we reduce the need for postoperative drops saving patients hundreds of dollars and hours of frustration, inconvenience and aggravation.
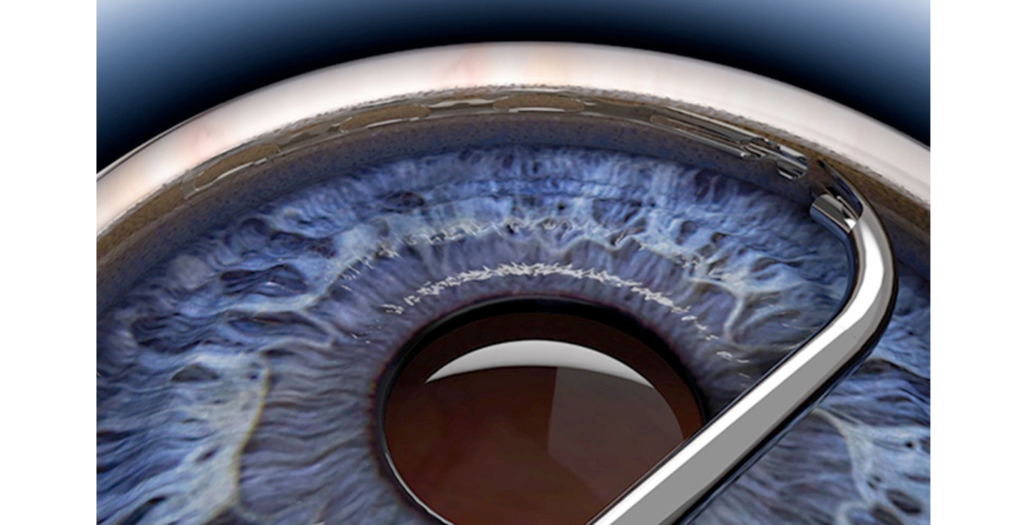
Hydrus MicroStent: Cataracts and Glaucoma
Stop your glaucoma drops with Hydrus MicroStent
Hydrus MicroStent has emerged as the best surgical option for patients with cataracts and mild to moderated glaucoma. Unlike some alternative MIGS procedures, Hydrus has been shown to reduce the risk of aggressive glaucoma progression. Nearly 80% of patients using a single drops each night can stop their glaucoma medication. Our practice is the most experienced in Pennsylvania with Hydrus. We serve as a training site for other surgeons and clinical specialists.
The Surgery Center at Fort Washington
A boutique surgical center with a convenient location.
467 Pennsylvania Ave, Suite 108
Fort Washington, PA 19034


















Patients Testimonials
Bob

Jeffrey H.
Ken O.

Louis
Yvette D.
Felicia W.
Jacqueline M.
Annie W.
Harriet L.
Mary V.
Louise & Arthur
Arthur
Kathryn H
Saul A.
Five Stars

John Y.
Rosemary M.
David C.
Peter
Ruth H.
Mary V.
Barbara
Wendy G.
Elizabeth N.
Barbara & Carl
Joyce G.
Olive G.
Glen M.
Stephen S.
Debbie J.
Avid D.
Christopher A.
Vivian C.
Anonymous
Ken O.
Anonymous
William
Tanya Y.
Shobhana & Monica S.
Bill